the pitt season 2 opened a conversation that felt less like fiction and more like an urgent mirror: episode 11 centers on Immigration and Customs Enforcement agents entering an emergency room, a detainee brought in with scant medical information, and a chain reaction that ends with a nurse detained. The episode’s timing and mechanics—written more than a year before recent escalations—have created a disconcerting overlap between scripted drama and unfolding events.
Why this matters right now
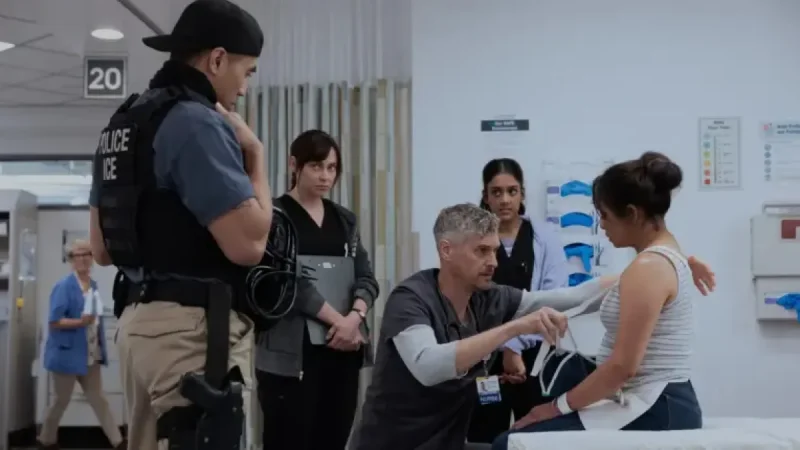
The episode landed amid a national debate over enforcement practices and hospital access. In the storyline, ICE agents bring a detainee to the emergency room and offer only that she fell, a minimal medical account that leaves staff and patients uneasy; several people leave the ER, and a staff member who intervenes is detained. Those plot points resonate against a backdrop in which ICE has been under scrutiny for enforcement actions, mass deportations and clashes that have had fatal consequences for individuals including Renee Good and Alex Pretti. That resonance is compounded by the fact that creators say the episode was scripted long before recent high-profile incidents, underscoring how on-the-ground reporting from clinicians fed into writers’ rooms.
Deep analysis: The Pitt Season 2 and the ICE storyline
Episode 11, titled “5: 00 p. m.,” deploys a compressed set of scenes to show how law-enforcement presence in a clinical setting can ripple outward. The dramatic beats are specific: an underinformed transfer, visible discomfort among patients and staff, an on-screen stand-off between Dr. Michael “Robby” Robinavitch and an agent, and the detention of nurse Jesse after he intervenes. Those concrete narrative choices highlight three connected dynamics: gaps in clinical information when custody transfers occur; the chilling effect on care-seeking behavior when enforcement is present; and the moral calculus faced by clinicians who must choose between de-escalation and advocacy for a patient.
Show leadership framed those choices as rooted in research and frontline consultation. R. Scott Gemmill, creator of the show, said, “this episode was written quite a while ago, before things got as escalated as they have. ” He described an iterative research practice—hosting a “nurses night” that brought 12 nurses into the writers’ process to identify pressing clinical and ethical tensions—and signaled ongoing outreach to residents and other staff. Gemmill added, “Of course, things have escalated beyond what they could’ve imagined, with things rapidly changing every day, ” a remark that captures the disconnect between the lead time required to write episodic television and the accelerating pace of real-world developments.



The program’s recent track record amplifies the effect. Earlier in the season, a measles outbreak storyline aired the same week cases began to accelerate nationally; that earlier coincidence, paired with this ICE-focused hour, suggests a sustained editorial aim to dramatize real systemic pressures on emergency medicine while relying on clinician input to shape narratives.
Expert perspectives and regional impact
Noah Wyle, the actor at the center of the series who portrays Dr. Robby Robinavitch, is part of a creative team that regularly consults medical professionals to reflect industry realities. John Wells, credited as an executive producer on the series, and the production’s research routines are presented as structural safeguards meant to keep dramatization tethered to clinician experience. Ned Brower’s character, nurse Jesse, is used narratively to show what can happen when a caregiver steps beyond clinical boundaries to protect a patient.
Those creative decisions carry regional and institutional import. Emergency departments operate as safety nets; disruptions that deter patients and staff from engaging with care can have cascading effects on community health, staffing strain and trust in medical institutions. The episode’s choreography—agents entering a public hospital space with incomplete medical information—models a worst-case interaction that clinicians and administrators must anticipate when balancing public-safety mandates against clinical confidentiality and patient welfare.
On a broader scale, the episode reframes a policy conversation as a bedside problem: enforcement activity is not an abstract statistic when it changes who walks into the emergency room, who remains in waiting areas, and who feels safe seeking care. That reframing makes the show less a timely coincidence and more a narrative intervention aimed at illustrating systemic consequences in a concrete setting.
As networks between policy and bedside practice grow tauter, the question persists: will dramatized portrayals like this episode prompt institutional adjustments in hospitals, or will they primarily serve as cultural touchstones that reflect existing anxieties? For viewers and health leaders watching both fiction and the news, the pitt season 2 episode forces that question into the open—what steps will hospitals and policy makers take next to protect access to care when enforcement meets emergency medicine?